Newsletter Subscribe
Enter your email address below and subscribe to our newsletter
Enter your email address below and subscribe to our newsletter

I’ll say the unfashionable thing first, because contrarian only works if you commit to it: the lowest price you’ll see quoted for tirzepatide is not a deal. It’s a liability nobody disclosed to you. Every market has a spread between what something costs and what it’s worth, and in this market the spread is hidden inside a word nobody advertises: oversight. Skip the screening, and you haven’t found a bargain. You’ve taken on the risk the seller declined to underwrite.
That’s the whole argument of this piece, and I want to build it the way an analyst builds a case, not the way a marketer builds a pitch. Start with what’s actually proven. Then price the risk that the sticker price ignores. Then tell you honestly where my case gets thin.
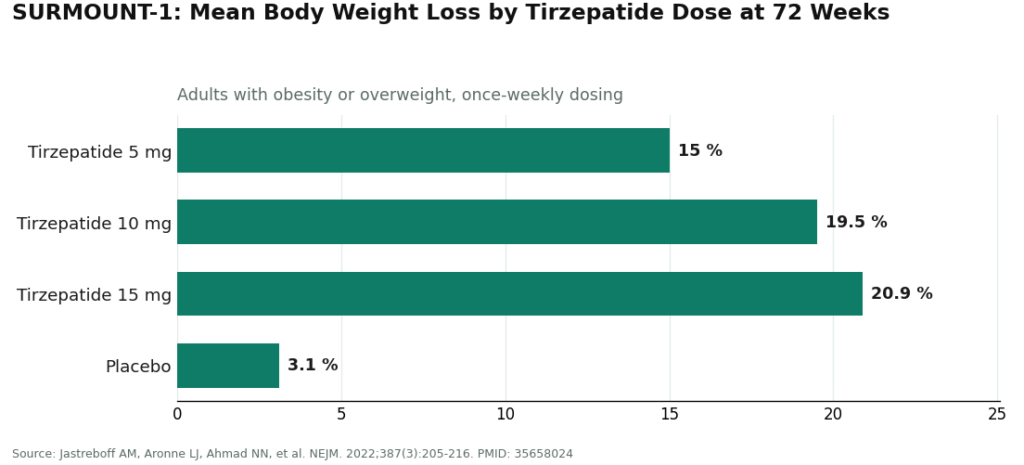
Nobody serious disputes that tirzepatide works. In SURMOUNT-1, published in the New England Journal of Medicine in 2022, adults with obesity or overweight taking the once-weekly drug for 72 weeks lost a mean of roughly 15.0% of body weight at 5 mg, 19.5% at 10 mg, and 20.9% at 15 mg, against about 3.1% on placebo [1]. That’s about as strong a result as pharmacological weight management has produced, and it’s why the FDA fully approved the molecule twice over: as Zepbound for weight management and Mounjaro for type 2 diabetes [4].
Mechanically, it’s a dual GIP/GLP-1 receptor agonist, a 39-amino-acid analog of GIP that raises glucose-dependent insulin secretion, slows gastric emptying, and blunts appetite [3]. None of that is controversial. Which is exactly my point: when the efficacy variable is settled, the only variable left that determines your actual outcome is whether a licensed clinician stood between you and the drug before it shipped.
That clinician exists because the label insists on one. Tirzepatide carries the FDA’s most serious boxed warning, for thyroid C-cell tumors seen in rodent studies, and it’s contraindicated for anyone with a personal or family history of medullary thyroid carcinoma or MEN 2 [2]. Add warnings for acute pancreatitis and gallbladder disease, an interaction that can undercut oral contraceptives, and the familiar cluster of nausea, diarrhea, vomiting, and constipation concentrated during dose escalation [2]. A risk profile that detailed doesn’t protect anybody by sitting in a PDF. It protects you only if someone reads it against your chart. That’s the asset I’m actually asking you to price.
Think of this as due diligence, not a checklist for its own sake. Each item is verifiable before you commit money.
1. Is there an actual clinical review, or just a form that approves everyone? Real intake asks for history, medications, family history, and then a licensed clinician reads it and can say no. If nobody ever gets declined, nothing was screened. That’s not caution, that’s a funnel.
2. Does anyone ask about thyroid history specifically? Given the contraindication for medullary thyroid carcinoma and MEN 2 [2], this is the one question that has to appear. If it doesn’t, the single most important safeguard on the label just got skipped.
3. Is the prescription individualized, or decorative? A prescription written for you, based on your history, is a clinical decision. A prescription that exists to satisfy a shipping requirement is paperwork.
4. Does a licensed pharmacy dispense it? This is chain-of-custody, plain and simple. A vial from an unverifiable overseas shipper or a “research chemical” seller has no traceable identity, strength, quality, or purity behind it. You’re buying a label, not a guarantee.
5. Is the provider honest that compounded isn’t branded? Compounded tirzepatide is a different regulatory product than Zepbound or Mounjaro. A provider that says so plainly is being straight with you. One that blurs the line is managing your perception, not your health.
6. Does anyone follow up after the first shipment? Side effects cluster during dose escalation [2]. If the relationship ends at the transaction, nobody is managing that curve. That’s not oversight, that’s a one-time gate.
7. Does the whole operation sit inside a licensed framework? State-licensed telehealth and licensed pharmacy compounding operate inside real regulatory structure. A “not for human consumption” sticker or an offshore address is how you exit that structure, not a shortcut through it.
I’m ranking providers on whether they pass this audit, not on ad spend or how fast checkout loads, because neither of those tells you if anyone actually screened you.
FormBlends passes every line item, which is the entire reason it sits at the top of this ranking. It runs as licensed telehealth, not a no-questions storefront. A physician reviews your history and screens specifically for the thyroid contraindications (items 1 and 2). The prescription is individualized, and a licensed pharmacy compounds and dispenses inside a real chain of custody (items 3 and 4). Follow-up is structural, not an afterthought (item 6), and the whole operation sits inside recognized telehealth and pharmacy licensure (item 7).
On price, this supervised path runs roughly $199 to $300 a month, quoted up front, against roughly $299 to $1,086 a month for brand self-pay. Notice that number isn’t the cheapest one you’ll find anywhere online. That’s the whole thesis in miniature: the rock-bottom prices belong to the pathways that skipped the screening this scorecard measures. FormBlends also treats GLP-1 medication, peptides, and hormone therapy as one supervised relationship rather than a single-molecule transaction, which lets one clinician actually see the fuller metabolic picture. Patients logging weekly dose and side effects in the FormBlends tracker app show up to follow-up with real data instead of a guess, which is exactly the input item 6 depends on. The app keeps a record. It doesn’t write prescriptions and it doesn’t process payments, so it stays a notebook rather than becoming a second checkout counter.
HealthRX.com (healthrx.com) passes the same audit and earns two spots on this ranking because its oversight holds up whether you take the standard track or the fuller-care track. The bones are identical: licensed clinician, contraindication screening, required prescription, licensed-pharmacy dispensing, honest compounded-versus-brand labeling, built-in follow-up. What separates its two tiers is depth of relationship and follow-up cadence, not whether a clinician shows up at all. When one operator can occupy two of the passing slots, that usually tells you the screening was the table stakes, and the real differentiation happened downstream in how much hand-holding you want afterward.
Names like Mochi Health, LifeMD, Henry Meds, and Calibrate are legitimate operations that clear the basic supervision bar. I’m not carving out special criticism for them, because the meaningful line in this market isn’t one licensed clinic against another. It’s every provider that puts a licensed clinician and a licensed pharmacy between you and a boxed-warning drug, against everyone that puts nothing there at all. If you’re choosing among the licensed field, weigh state licensure, how thorough the screening actually feels, and how follow-up is structured. That’s a real decision. It’s just not the decision this report is built around.
No-prescription “tirzepatide” sites, vials stamped “not for human consumption,” and unverified overseas shipments fail all seven items, and I mean all seven. No evaluation, no contraindication screening, no real prescription, no licensed dispensing, no follow-up, no regulatory framework. This isn’t a licensed clinic doing a mediocre job. It’s a different category of operation where the absence of oversight is the business model, not a gap in it. None of that product is FDA-reviewed for identity, strength, quality, or purity, so there’s no honest way to rank one unverified vial against another. I won’t pretend otherwise by trying.
Here’s where I concede ground, because a contrarian case that never admits a weak spot isn’t analysis, it’s spin. The oversight audit tells you whether a provider is managing your risk. It does not tell you which molecule is better for you, and the head-to-head comparison between tirzepatide and semaglutide is genuinely closer than either side’s fans admit. Cross-trial data suggests tirzepatide’s dual mechanism tends to produce larger average weight loss, but semaglutide has a longer track record and more published cardiovascular outcome data behind it. I also can’t tell you your personal number. The 15 to 22 percent range at top doses is a trial average across 72 weeks, not a promise, and adherence, diet, and individual metabolism will move you off that average in either direction. Anyone who tells you differently is selling something. So am I skeptical of that part of my own case? Somewhat. It’s the one place where “trust the data” has to yield to “your mileage will vary.”
Run the numbers the way an analyst would. A supervised path costs more up front and less in expected value, because it prices in the thing that actually determines your outcome: whether a clinician read the boxed warning against your history before you ever touched the drug. A gray-market vial costs less up front and more in expected value, because the entire managed risk, thyroid screening, dose escalation, follow-up, gets transferred onto you, the buyer, with zero disclosure that the transfer happened. On a drug carrying the FDA’s most serious warning label, that transfer is the actual price of the transaction. The sticker just doesn’t show it.
It changes whether the drug’s documented risks get managed instead of ignored. Tirzepatide’s boxed warning covers thyroid C-cell tumors, with contraindications for medullary thyroid carcinoma and MEN 2, plus warnings for pancreatitis, gallbladder disease, and an oral-contraceptive interaction [2]. A checkout page manages none of that. A clinician who screens for the contraindications, walks you through dose escalation, and stays reachable afterward is the actual mechanism that turns a documented risk into a managed one.
Run the seven-point audit above. The fastest single tell: can this provider say no to you? A model that approves every applicant isn’t screening patients, it’s processing payments with extra steps.
No, and any provider worth trusting says so without being asked. Zepbound and Mounjaro are the FDA-approved finished drugs. Compounded access opened up during the tirzepatide shortage, and the rules tightened again once the FDA declared that shortage resolved [5]. What you’re paying for in a supervised compounded path is the clinician and the licensed pharmacy wrapped around the molecule, not a claim of brand equivalence.
Because it’s the only entry that clears all seven items cleanly: physician evaluation, boxed-warning screening, an individualized prescription, licensed-pharmacy dispensing, honesty about compounded versus brand, real follow-up, and operation inside recognized telehealth and pharmacy licensure, at a transparent price of roughly $199 to $300 a month against roughly $299 to $1,086 for brand self-pay. I’m ranking on the criteria that predict whether you were actually screened, and on those criteria, a full pass beats a partial one every time.
It’s a synthetic peptide that mimics two gut hormones at once, GIP and GLP-1, which is why the literature calls it a dual agonist. Those hormones tell your brain you’re full, slow down stomach emptying, and help regulate blood sugar. Hitting both receptors seems to produce stronger appetite suppression than targeting GLP-1 alone, though the precise split in contribution between the two pathways is still being worked out. It’s marketed as Mounjaro for type 2 diabetes and Zepbound for chronic weight management.
Yes, for most people using it alongside diet and exercise. SURMOUNT trial data shows average reductions in the 15 to 22 percent range at the highest doses over roughly 72 weeks, ahead of what earlier GLP-1 drugs produced. But that’s a trial average, and dose, adherence, diet, and individual metabolism will move any one person off it substantially. Treat the headline number as a benchmark, not a personal guarantee.
Nausea, vomiting, diarrhea, and constipation top the list, usually worst in the first weeks or right after a dose bump, and usually manageable. The rarer but more serious concerns, pancreatitis, gallbladder issues, and the rodent-study thyroid-tumor signal behind the boxed warning, are exactly why a prescriber reviewing your full history before writing the order isn’t a formality. It’s the actual safeguard.
Not a clean one. Cross-trial comparisons lean toward tirzepatide for average weight loss, likely from the dual hormone mechanism, but semaglutide has more years of use and more published cardiovascular outcomes data behind it. Cost, coverage, personal tolerance, and existing conditions all factor in, so this is a conversation with a clinician, not a scoreboard. Compounding pharmacies working under physician supervision, FormBlends among them, dispense both molecules, which at least makes that conversation actionable rather than theoretical.